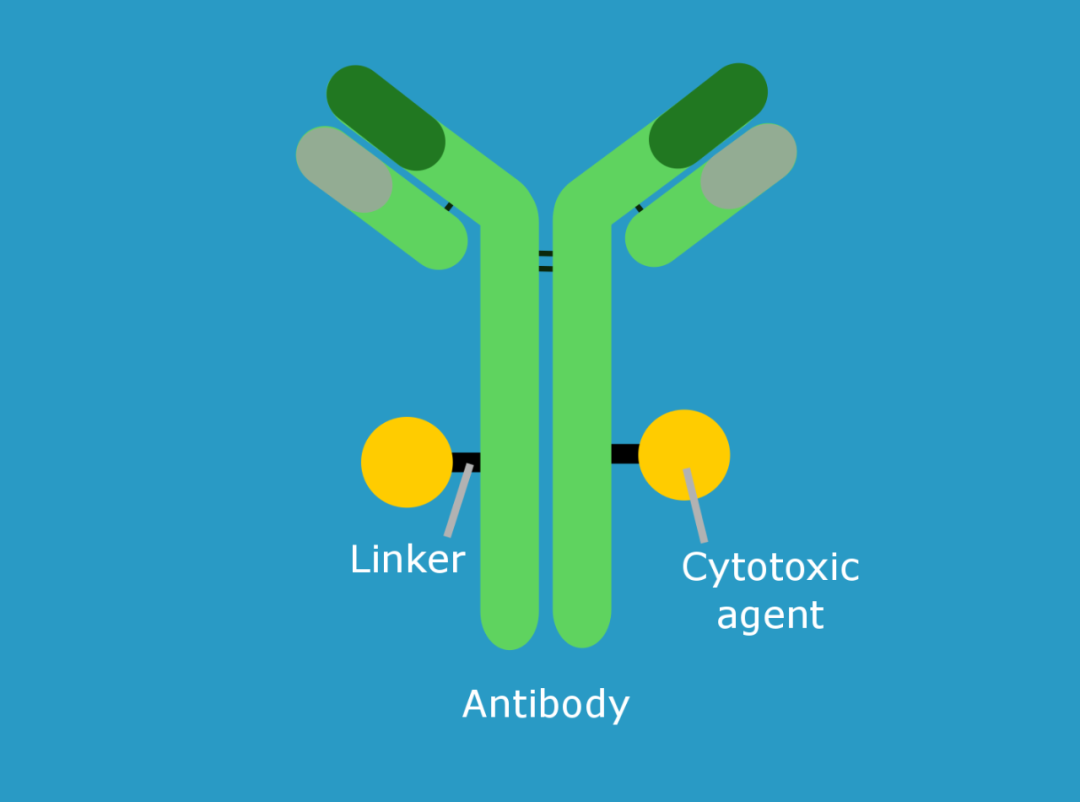
Structure is the key to achieving functionality. The structure of an ADC is obvious: antibody, linker, and coupled drug. Whether an ADC is successful or not, every component is important. The selection of the target and the quality of the antibody determine the affinity of the ADC to tumor cells; the type of linker determines the stability of the drug; the choice of the coupling drug determines the lethality and side effects of the ADC.
The “Y” shape is a typical antibody structure, and the “small red ball” dotted in it is the coupling drug. The linking part of the antibody and the drug is the linker. Antibodies help the ADC find tumor cells accurately, and then release the coupled drug. The tumor cells that were “medicated” eventually lost the power of the drug and “died”.
Therefore, the choice of target is very important. The target needs to be tumor cell specific. If the target is expressed in both tumor cells and normal cells, then ADCs and chemotherapeutics are the same. Second, the target must be expressed at least in large amounts in tumor cells and a small amount in normal cells, so as to reduce the “accidental injury rate”.
Linkers are also very important for ADCs. The stability of the linker determines its precise release and reduces “off-target effects”. Linkers are divided into two types: decomposable and non-decomposable. The ADC drug must remain stable when circulating in the body. After reaching the target cell, the coupled drug is released, giving the tumor cell a “fatal blow”.
The choice of coupling drugs, ie cytotoxic substances, is also extremely important. The toxicity is not enough, and the tumor cells can still live happily. The toxicity is too strong, and it is easy to “afflict the pond fish”. There are two main types of ADC toxic substances on the market today: one is the destruction of the DNA double helix, which makes tumor cells “severe hemiplegia and hemiplegia”; the other is anti-microtubule formation, which prevents tumor cells from normal mitosis.







